For the technician doing trans thoracic echo (TTE) you can greatly improve your regional wall motion abnormalities analysis (RWMA) using two rapids drawing of the left ventricle (LV) in order to do a 3 minutes concordance test.
These drawing are done while doing a regular trans thoracic echocardiography (TTE) .This test could be a useful teaching tool for trainees that begin to do routine TTE. It is a useful test in patients with TTE wall motion abnormalities. Hoping this will help some of you. Your comments and suggestions would be appreciate
Drawing
We do simple thing:
-You can use this technic in a restrict space with a plain sheet of paper and a pen.
-You need only a sheet of paper letter size (8 1/2”- 11”).
-You draw your patient short axis: Basal, Mid and Apical (BMA) and apical 2, 3, 4 chambers (234C) manually (10 sec).
-You can use this drawing or the preprinted example we did.
-You can fold the letter page and have 4 patients/sheet in your pocket (8 patients if you use both side).
* You can find the preprinted example sheet at the end of this document.
The two rapid drawing of the left ventricle should be done before or during the regular trans-thoracic echo.
Classical LV short axis
A 7 seconds drawing of the Basal segment (mitral valve), the Mid segment (papillary muscle) and the Apical segment. (BMA).
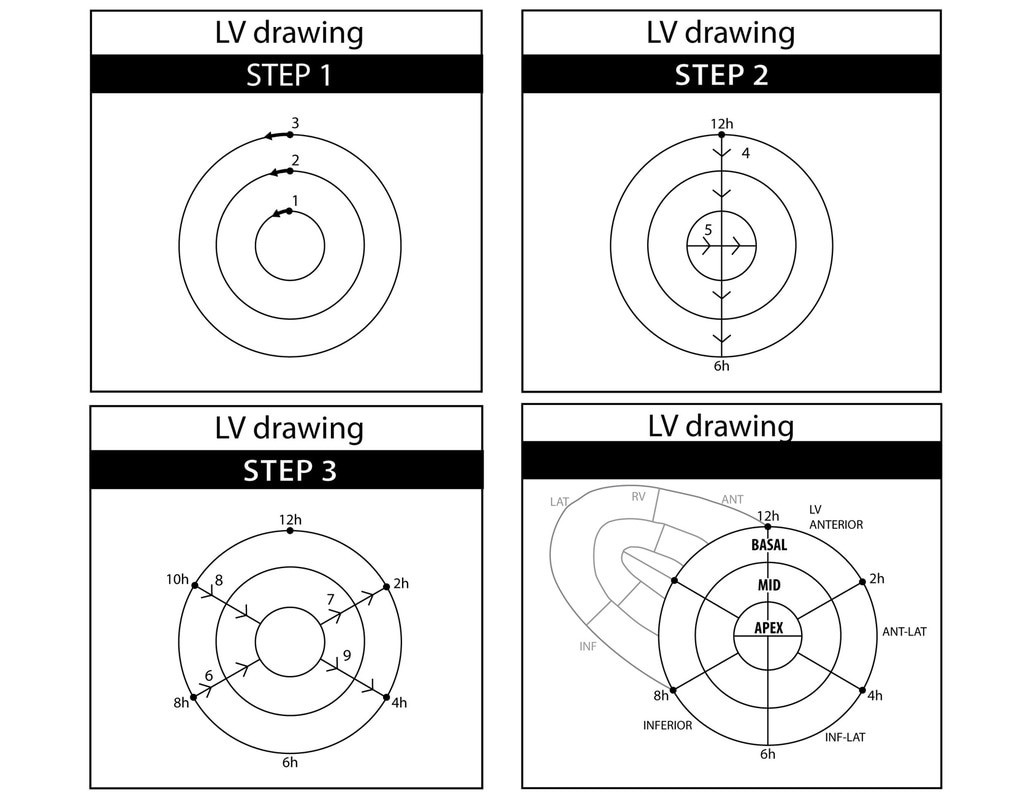
Fig.1 – Step 1 to 3.
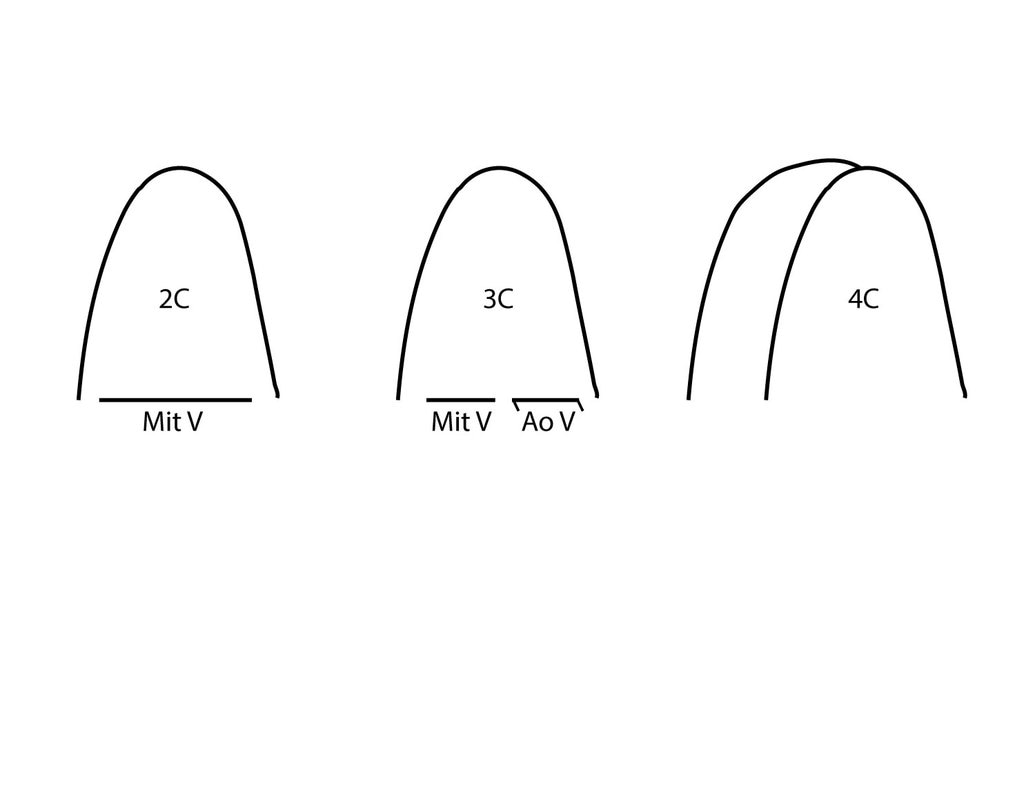
Classical LV apical
A 3 seconds drawing of the views 2 chambers, 3 chambers and 4 chambers. (234C).
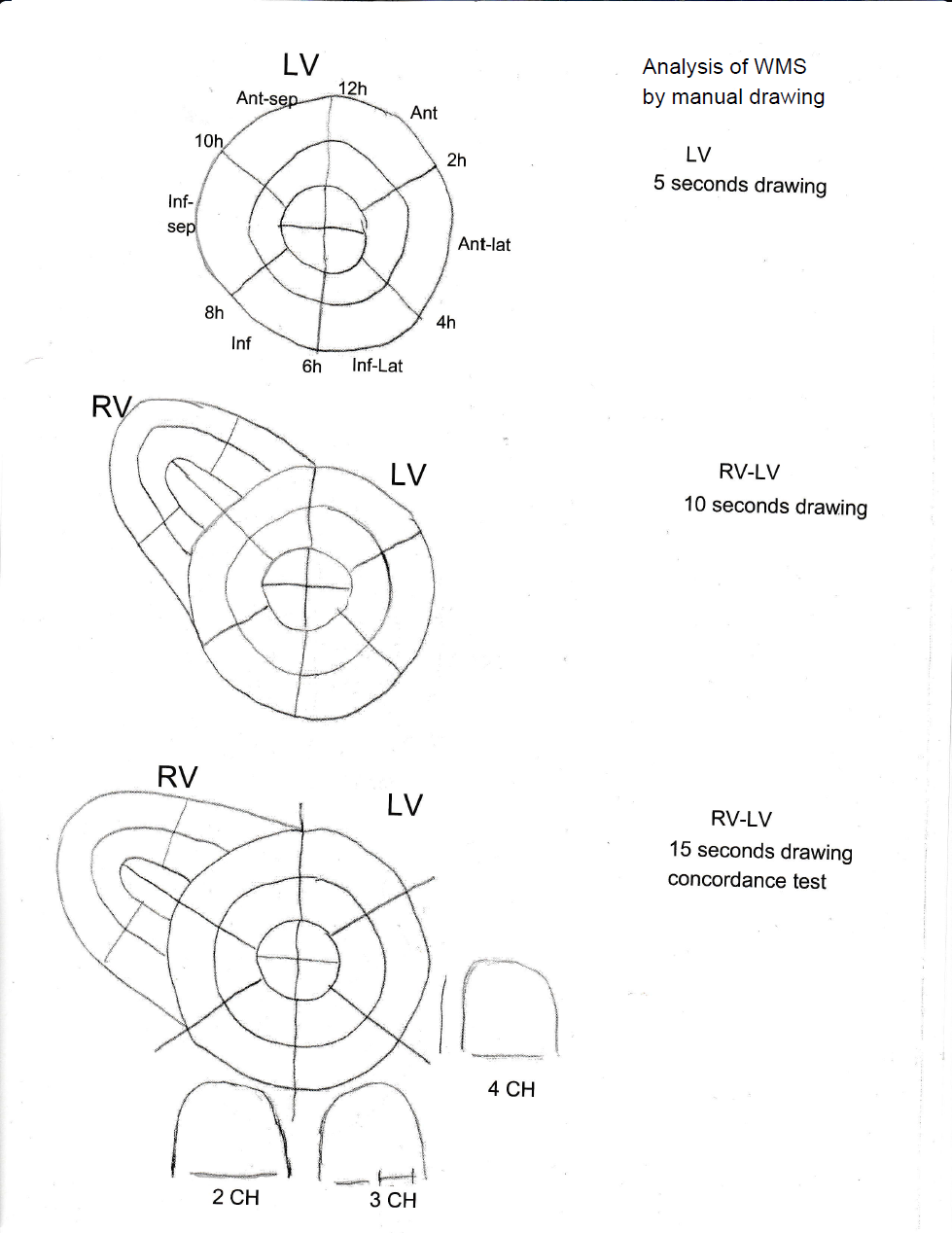
Example: A sample of an handmade drawing (Fig.3-4).
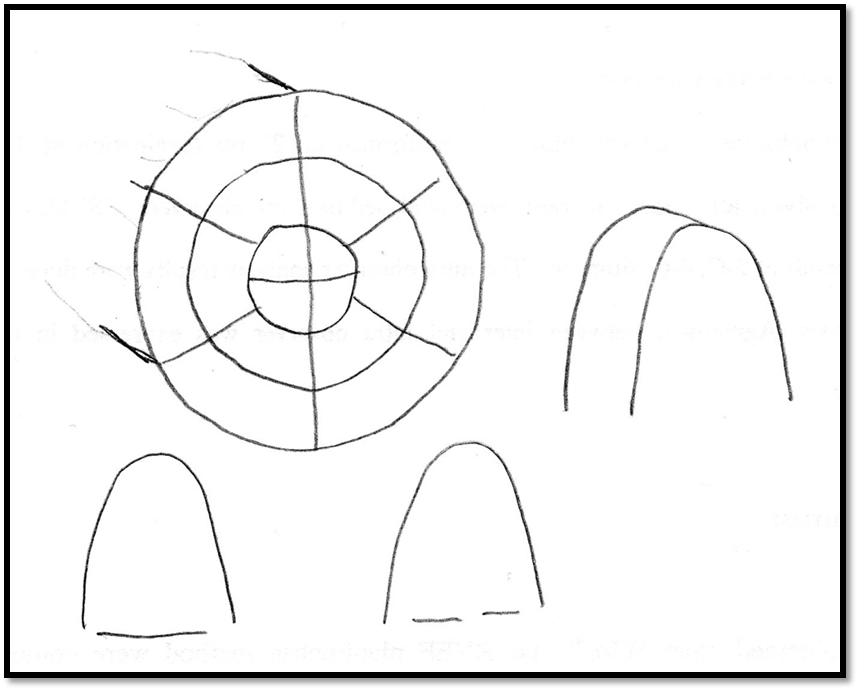
Fig.3 – Handmade example of a 10 seconds drawing.
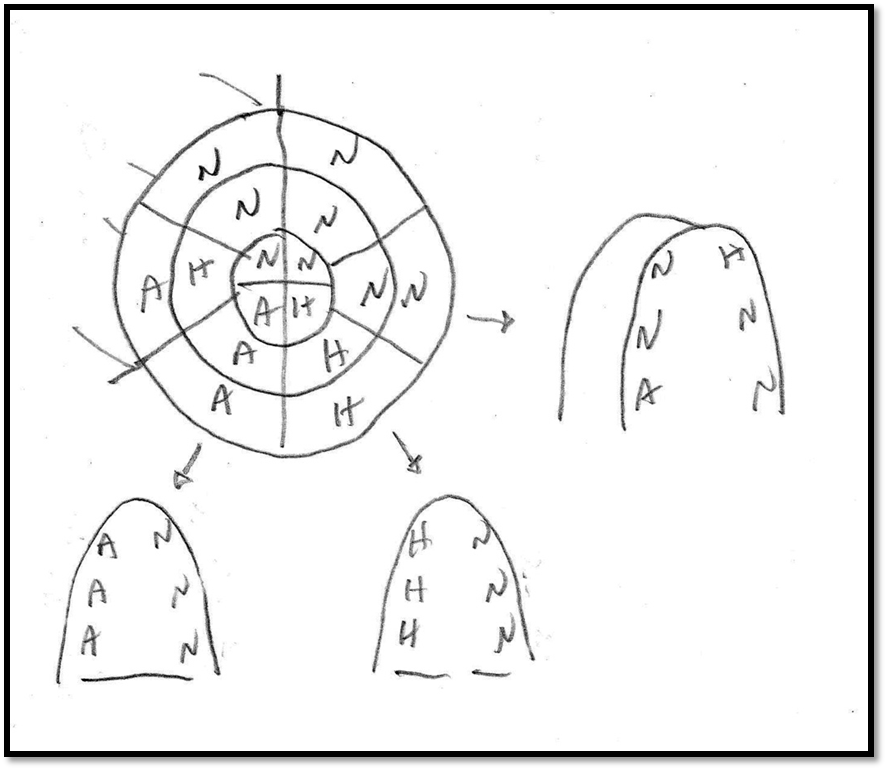
Fig.4 – Handmade example for an inferior infarction.
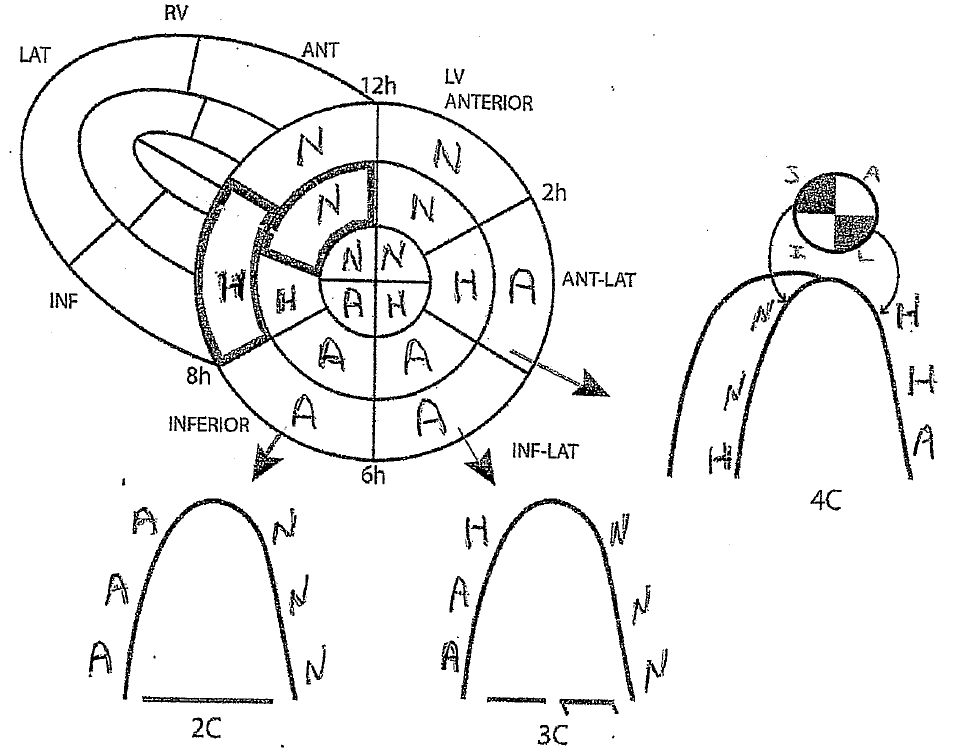
B- Anatomical correlation
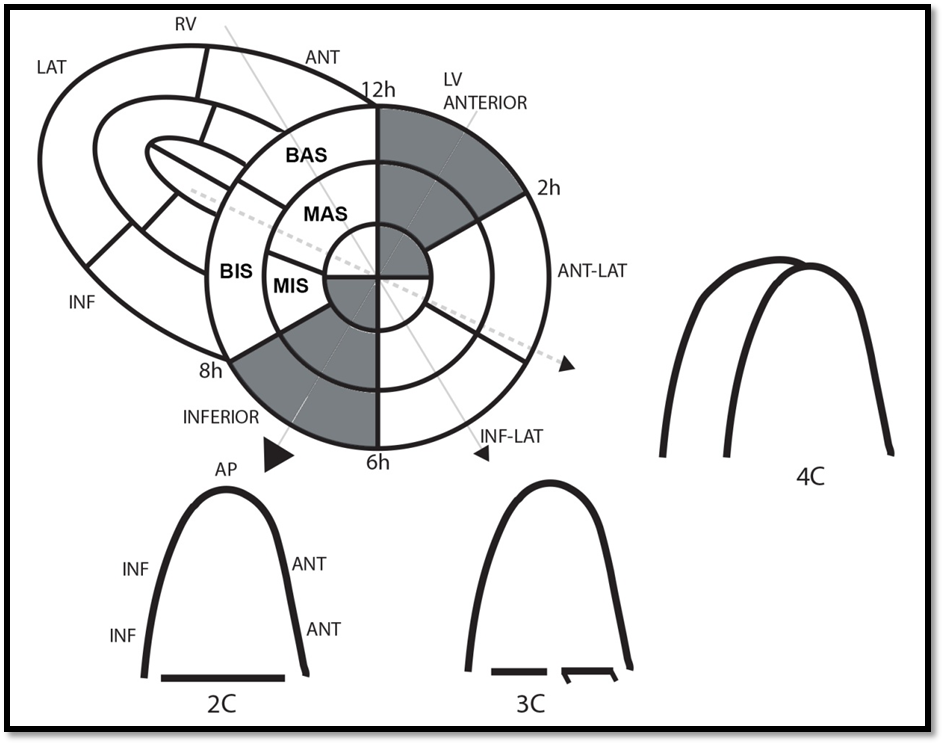
Fig.5 – Anatomical correlation between the 16 segment of the BMA and the 2C.
N.B.: the true 2C with 2 leaflets (cf: A systematic approach...)
BAS: Basal anterior septum
MAS: Mid anterior septum
BIS: Basal inferior septum
MIS: Mid inferior septum
I-L: Infero-lateral
A-L: Antero-lateral
INF: Inferior
ANT: Anterior
AP: Apex
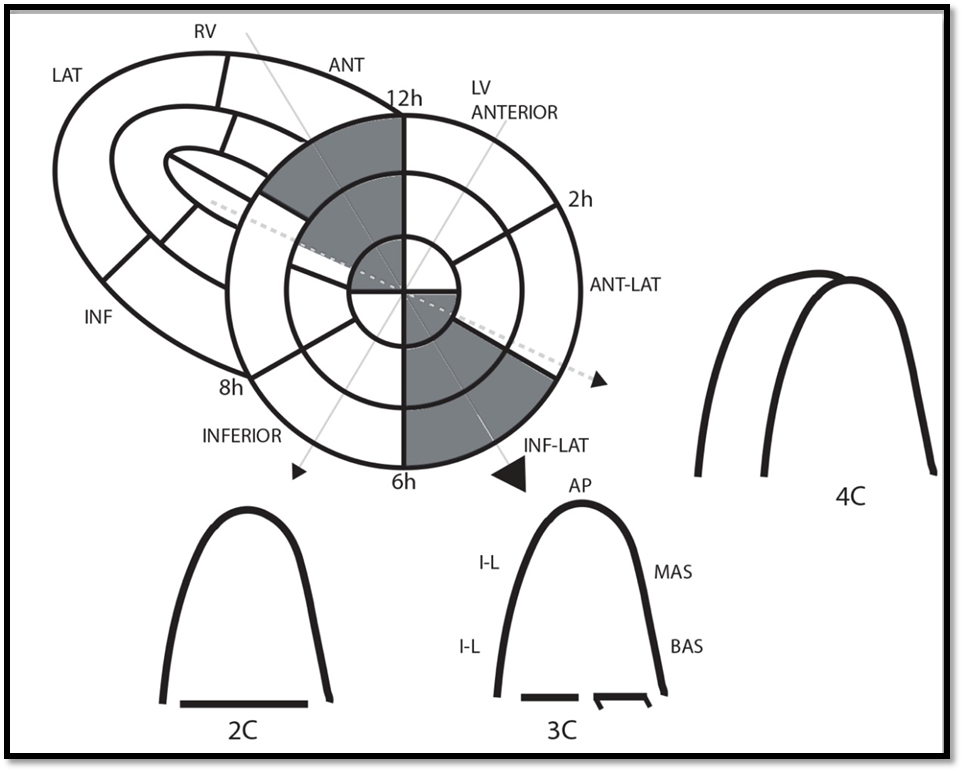
Fig.6 – Anatomical correlation between the 16 segment of the BMA and the 3C.
BAS: Basal anterior septum
MAS: Mid anterior septum
BIS: Basal inferior septum
MIS: Mid inferior septum
I-L: Infero-lateral
A-L: Antero-lateral
INF: Inferior
ANT: Anterior
AP: Apex
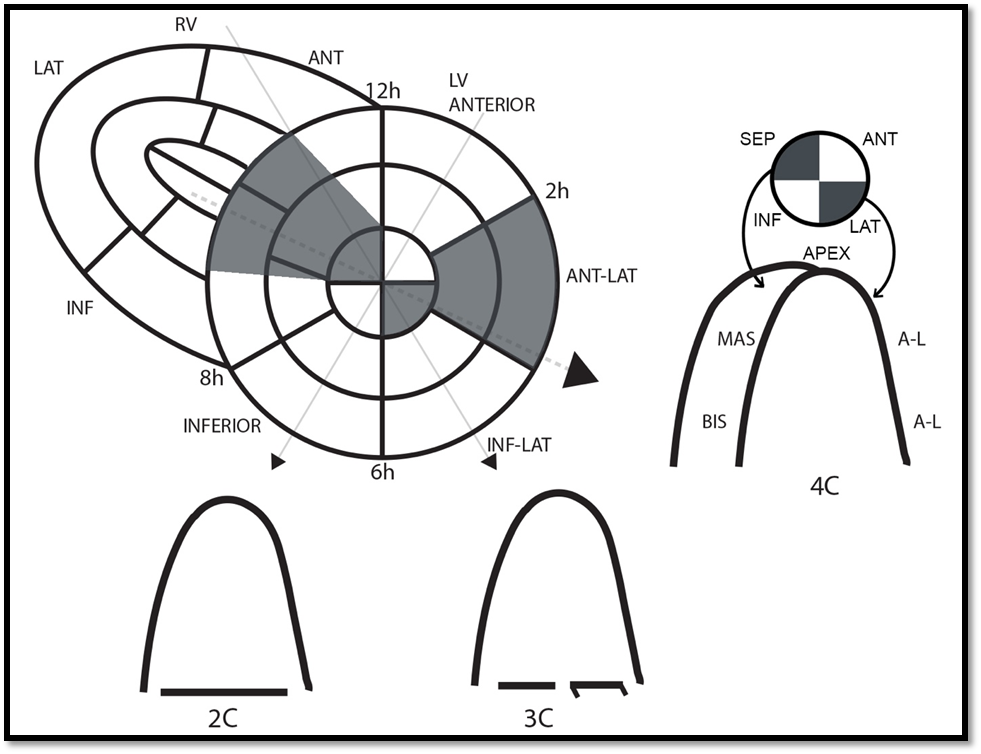
Fig. – 7 - Anatomical correlation between the 16 segment of the BMA and the 4C.
BAS: Basal anterior septum
MAS: Mid anterior septum
BIS: Basal inferior septum
MIS: Mid inferior septum
I-L: Infero-lateral
A-L: Antero-lateral
INF: Inferior
ANT: Anterior
AP: Apex

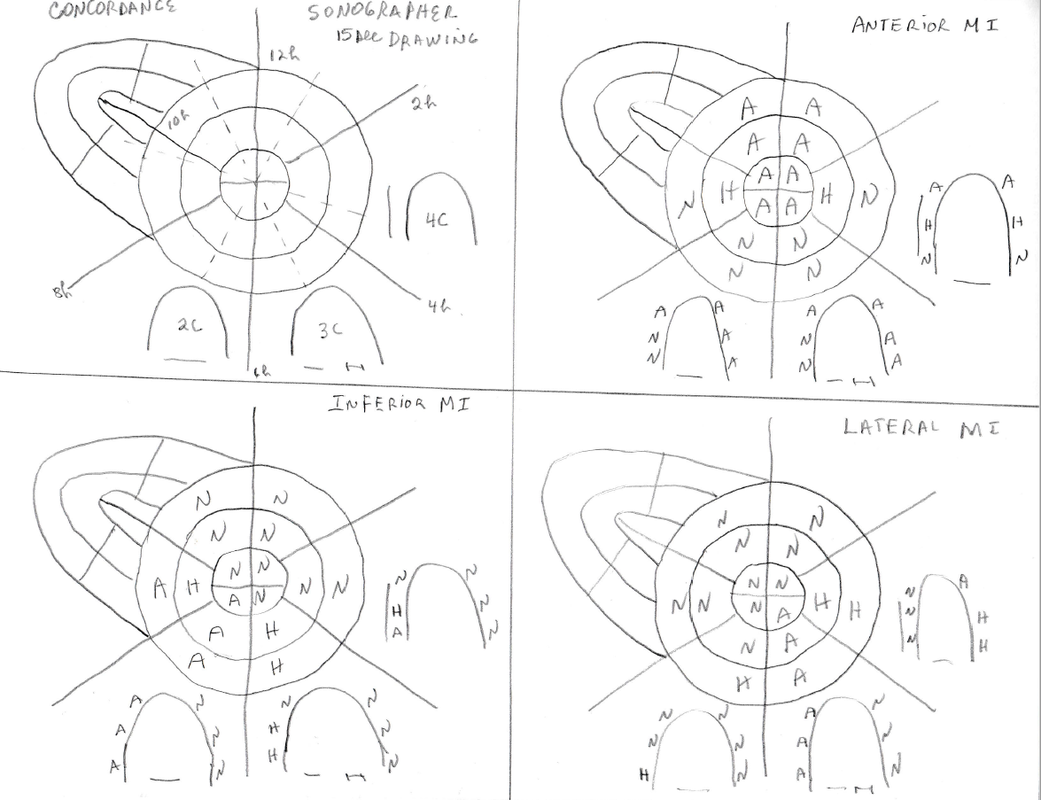
Fig.8 – Example of myocardial inferior infarction
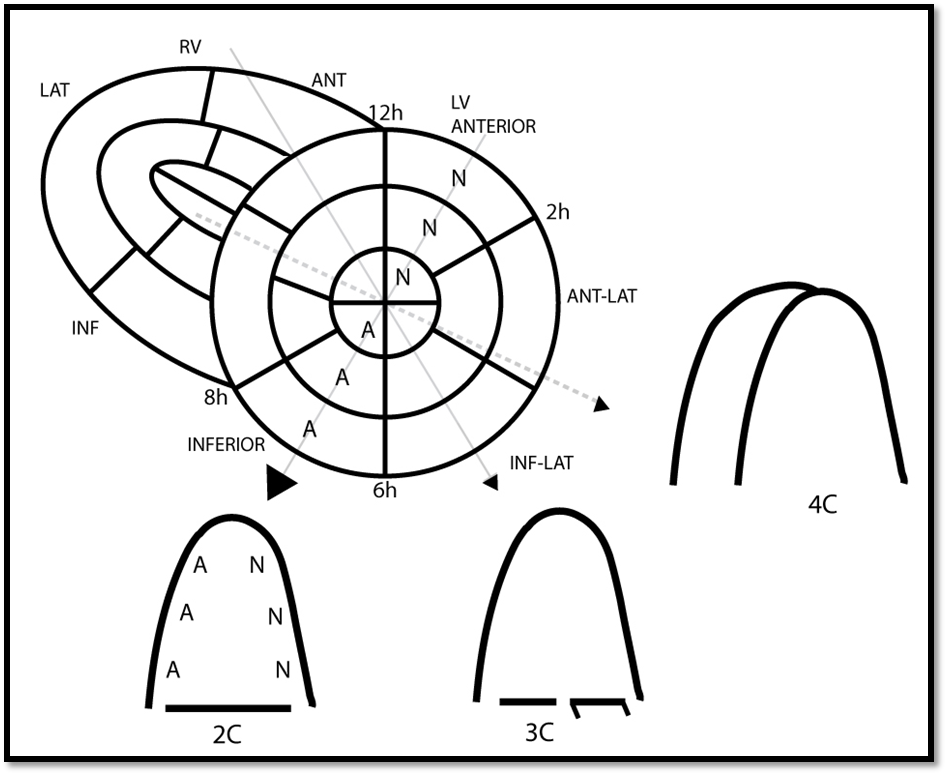
Fig.9 – Anatomic correlation BMA-2C
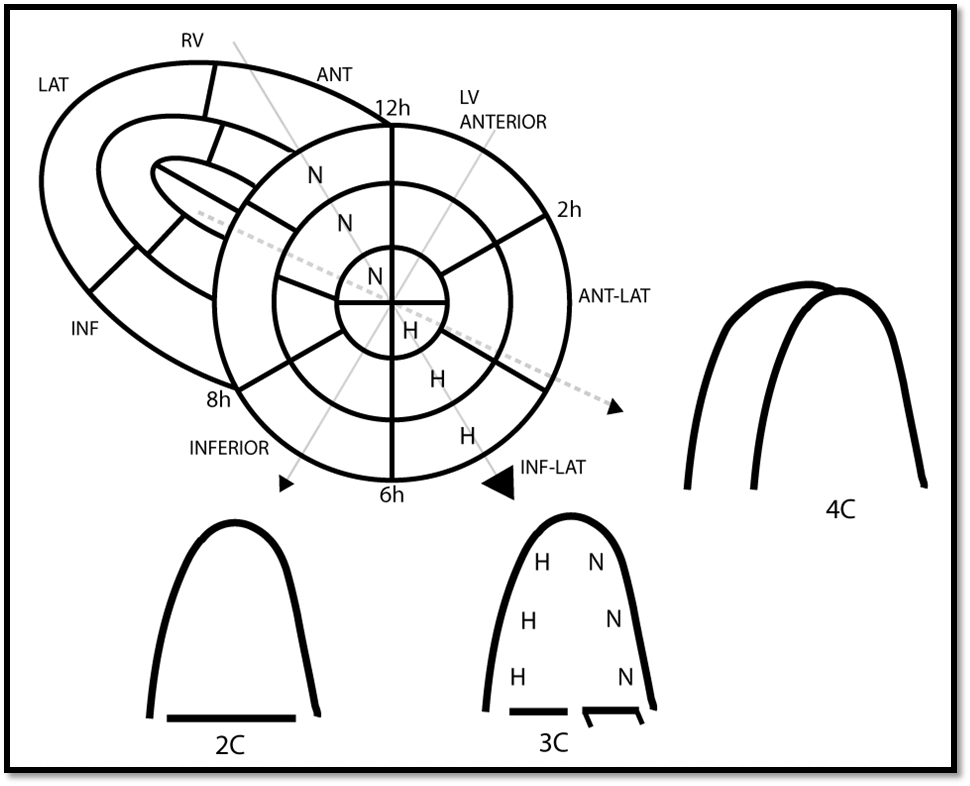
Fig.10 – Anatomic correlation BMA-3C
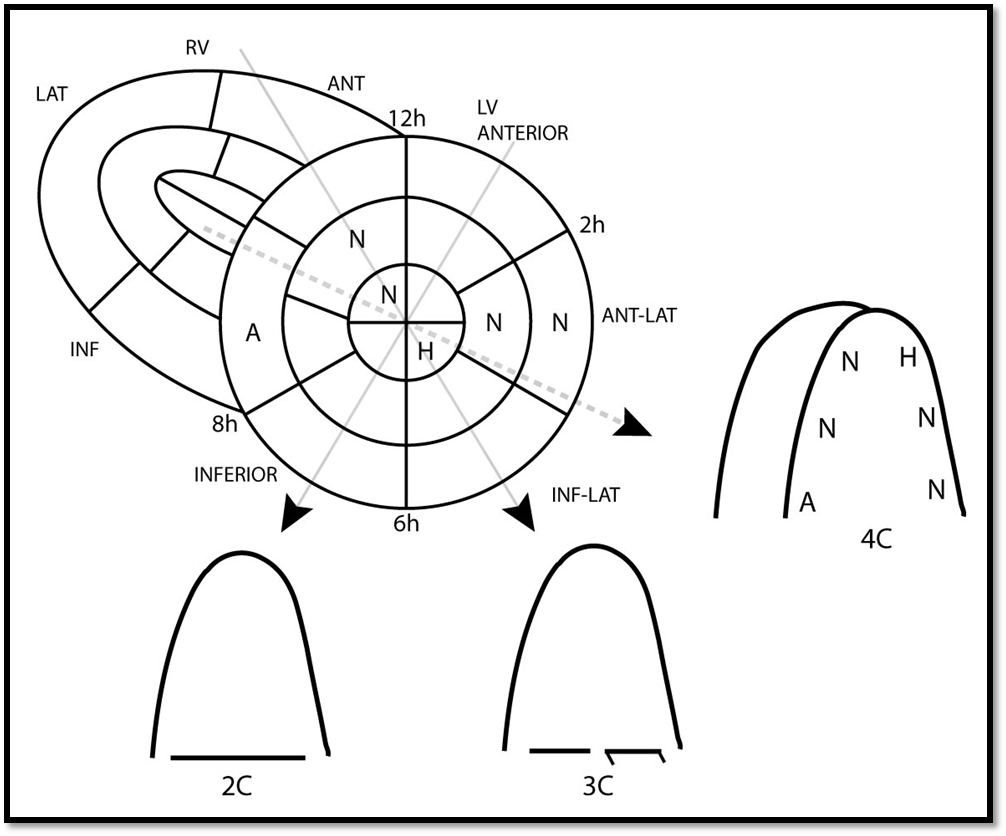
Fig.11 – Anatomic correlation BMA-4C
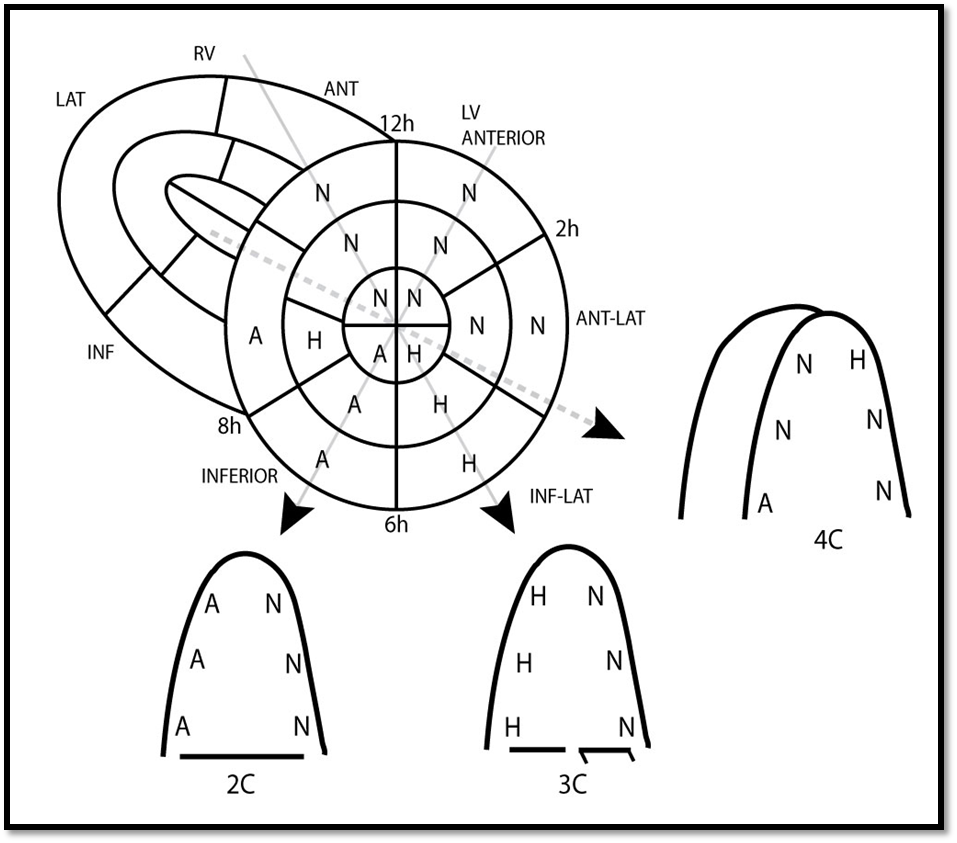
Fig.12 – 234C derived from BMA
The 2 and 3 chambers views are relatively simple to analyse as they easily correlate with their respective segments. Example of an inferior infarction.
The 4 chambers view is somewhat more challenging for the apex and the septal wall.
4C walls
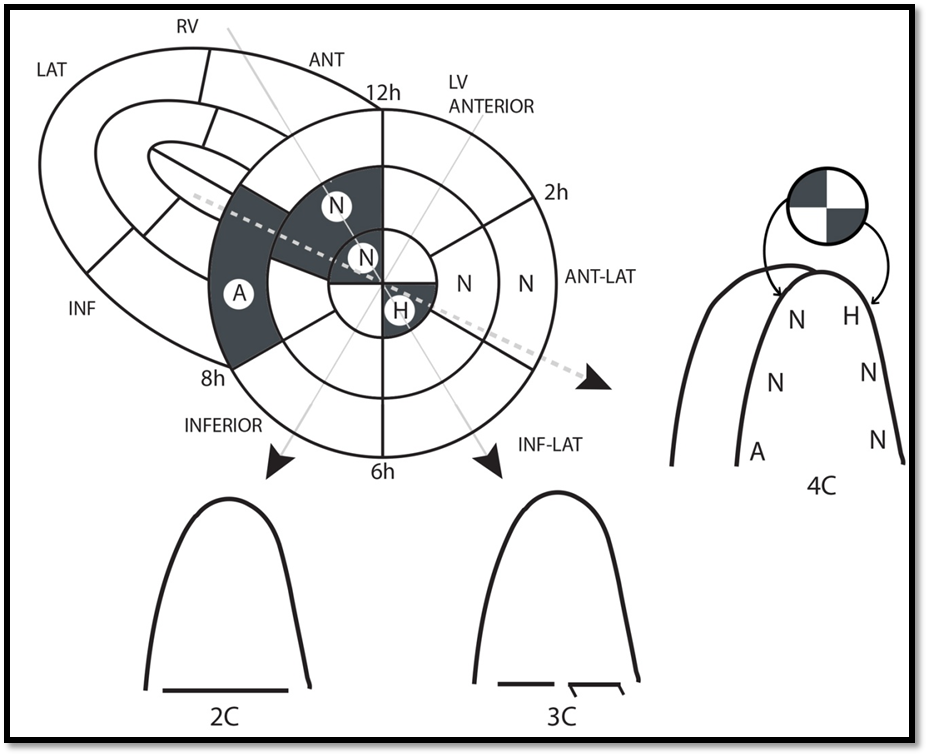
Fig.13 – 4C septal wall:
The basal septal wall of the classical 4C correlates with the basal inferior septum segment (BIS) of the BMA. This segment is generally dependant of the right coronary artery (RCA) circulation.
The basal inferior segment is longer than the basal anterior segment. The right coronary circulation cover a larger region in the basal septum than the LAD.
The mid septal wall of the 4C correlates with the mid anterior septum segment (MAS) of the BMA. This segment is generally dependant of the left anterior descending artery (LAD) circulation.
The mid anterior segment is longer than the mid inferior segment. The Left anterior descending circulation cover a larger region in the mid septum.
----- 4C lateral wall: lateral wall is generally the short axis antero-lateral wall
----- 4C Apical wall: Use the septal apical and lateral apical segment of the BMA for the 4C apex
You can confirm the 4-segment short axis of the apex using long axis and apical views
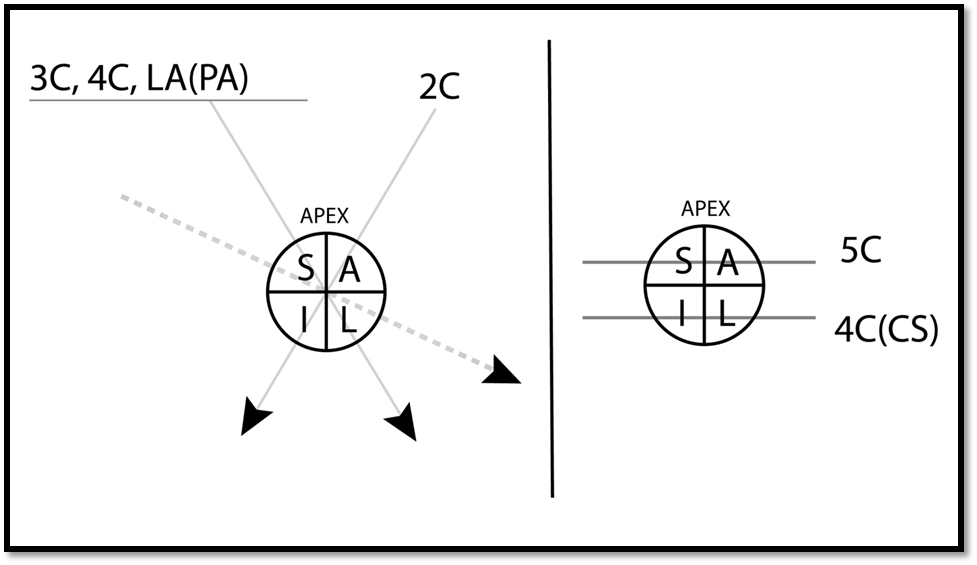
Fig.14 - LA(PA): long axis para-apical / 4C(CS): 4 chambers (coronary sinus)
COMMENTS
The variation of the 4C septal segment with angulation or rotation.
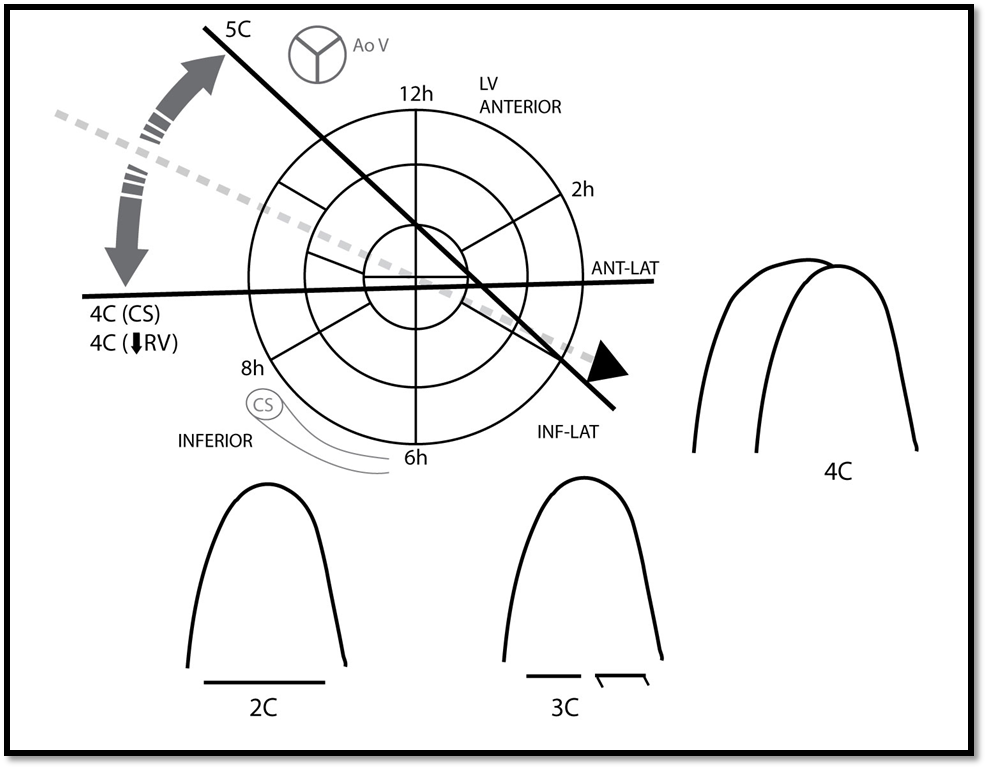
Fig.15
Upper orientation: gives 5C (BAS and MAS)
Lower orientation: gives 4C with coronary sinus (BIS and MIS).
rotation: 4C in rotation toward the 2C (with smaller RV) give BIS and MIS.
You can use this information to ameliorate your analysis of the 4C. Having your bull eye or polar map quotation in mind or in your drawing you can very rapidly check your BAS and MAS by simple upward angulation from your classical 4C to your apical 5C. You can check your BIS and MIS by simply downward angulation toward your low 4C with coronary sinus (CS) or rotation from the classical 4C to 4C with smaller RV.
Concordance test
Materiel needed: schematic drawing of BMA and 234C.
STEP 1: length 1-2mt
During the regular TTE after you have acquired your three classical short axis (BMA) for RWMA you fill up the Bull eye 16 segments. Do not wait at the end of exam often you will be short of time and the patient may be tired if you have to come back and do some image. We are not using routinely mild hypokinesia (MH) neither severe hypokinesia (SH).
A = akinesia H = hypokinesia N = normokinesia D = dyskinesia
AN= aneurysm MH= mild hypokinesia SH = severe hypokinesia
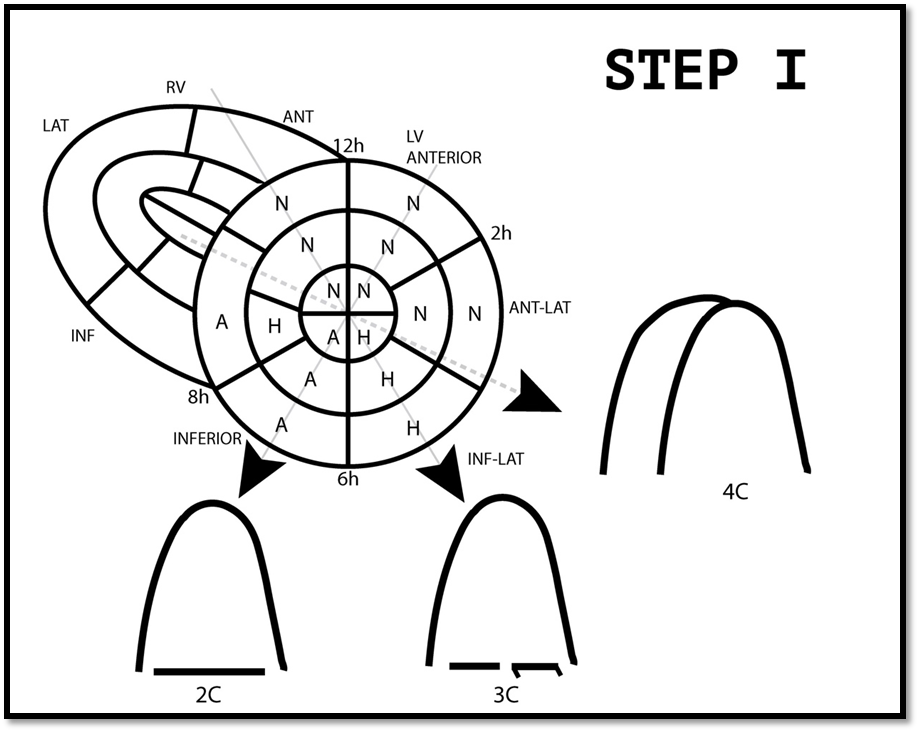
Fig. 16
STEP 2: length 20 sec.
Apply your segment analysis to the 234C drawing that correlate to each segment.
(inside drawing)
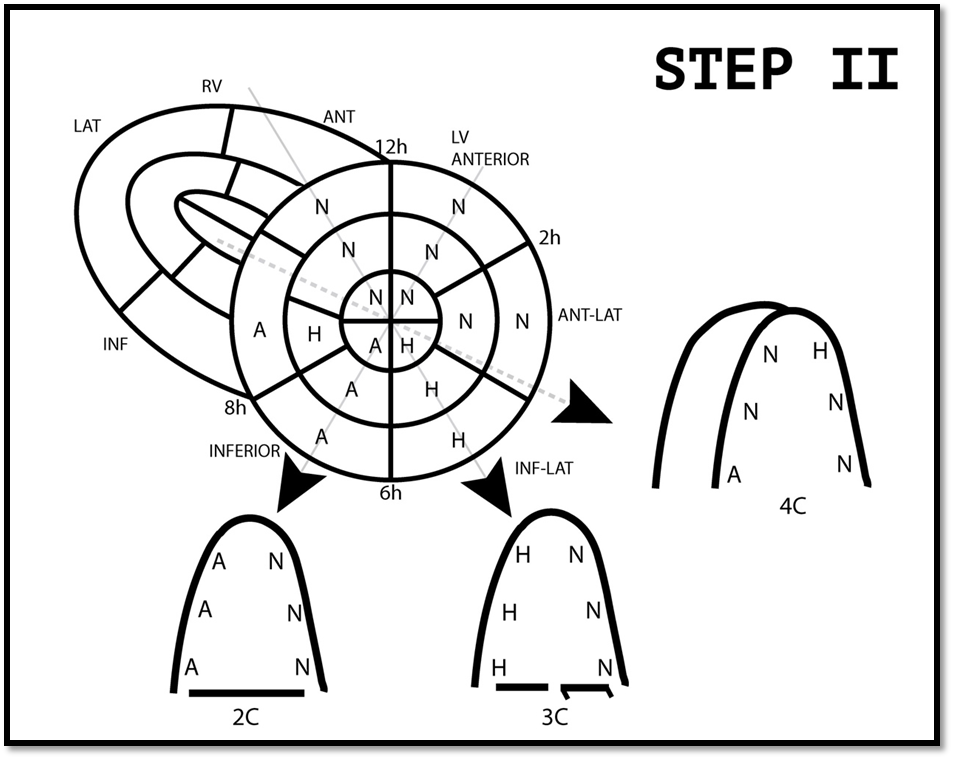
Fig. 17
STEP 3 – Concordance test (length 1-2mt)
After step 2 done you get your classical apical 2D views 234c and put them in the outside drawing of the 234c then you compare to the 234C views analysis prediction that you have written down in step 2 (inside drawing) with the apical views that you have obtain during your exam
(outside drawing).
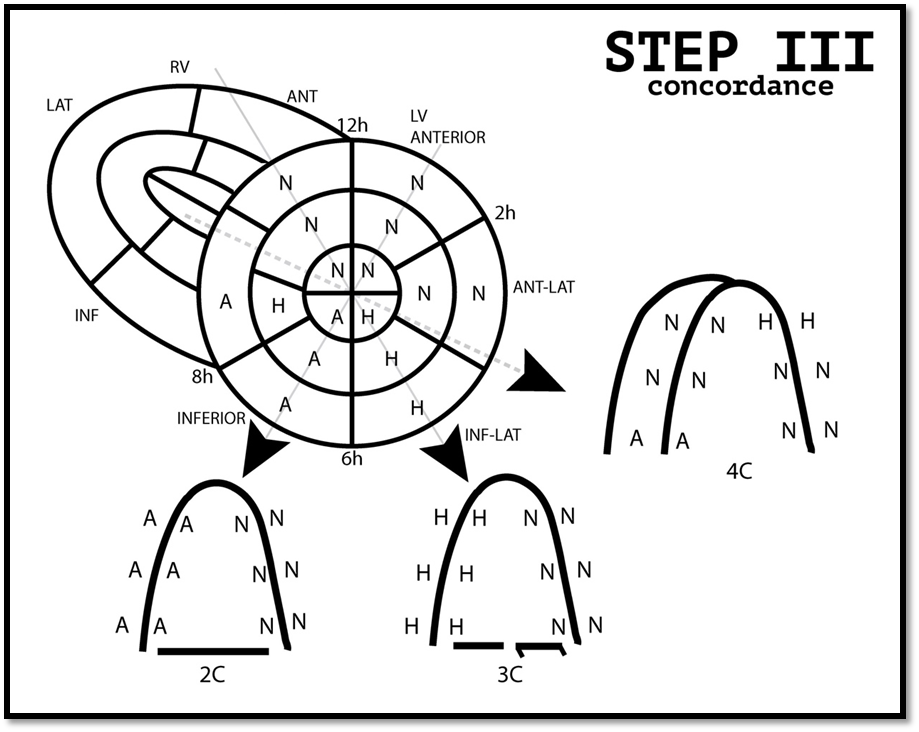
Fig. 18
If your segment analysis 234C (outside drawing) transposed to your step 2 drawing (inside drawing derived from the BMA) are concordant you have a concordant analysis.
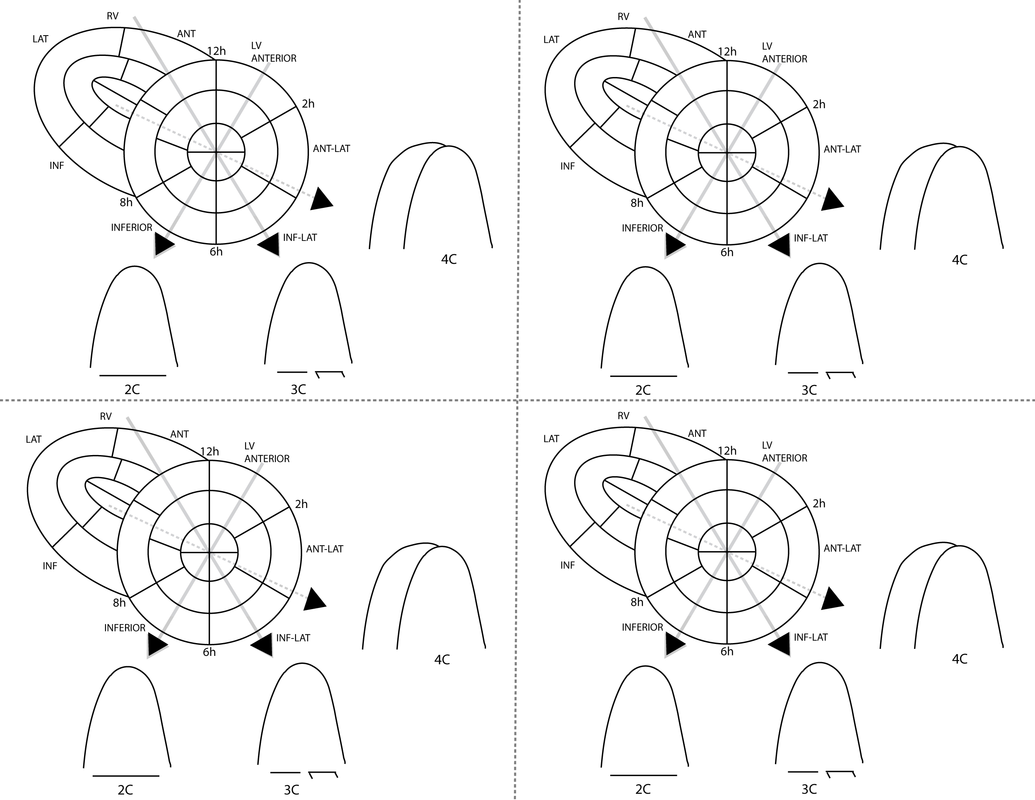
STEP 3 – Non-Concordance test
However, if your segment analysis 234C (outside drawing) transposed to your step 2 drawing (inside drawing derived from the BMA) do not corroborate you need to reanalyse the short axis or apical views so that the discordant segment may be corrected.

Fig. 19
Example of a severe non-concordance is a normal kinetic anterior wall in BMA and an akinetic anterior wall in 2C. A mild non-concordance would be a normal anterior wall kinetic in BMA and hypokinetic wall in 2C. After using the concordance test for a certain moment, you will skip step 2 and preview in your mind the correlation between BMA and 234C and you will understand the technical move that can explain non-concordance in certain situations.
COMMENTS.:
1- Every long axis with aortic valve is BAS and MAS (3C, 5C, long axis, long axis para apical and 5C subcostal).
Classical subcostal 4C gives BIS and MIS.
2- Classical Left para sternal long axis (third intercostals space near the sternal border) give a nice image on 2D (perpendicular to LV wall) of BAS, MAS and basal and mid inferolateral segments but no apex.
Apical 3C (near the apex impulse) give a nice view of the apex but the basal and mid segment are not as clear on 2D (parallel orientation to LV wall).
The long axis para apical (Fourth to fifth intercostal space at 5-10cm left of the sternal border) give you the best perpendicular septal anterior segments, inferolateral segments and perpendicular view of the apex.
3- Anatomic versus schematic drawing of the short axis of the LV.:
We put the RV- LV junction at 12hr in our drawing. In fact at the base the junction of RV-LV in your 2D image is more at 13hr , in the mid portion the junction is approximately at 12-12,30hr and at the apex section junction is around 11-12hr . For didactic purpose, we put the RV-LV junction at 12hr on our schematic representation.
4- For the RWMA kinetic analysis the 16 segments model is correct. For perfusion studies the 17 segments is preferable.
5- Apical views are essentials as short axis because the apical views are the best for evaluation of dyskinesia and aneurysm.
6- If para sternal short axis views are of poor quality you can complete the BMA Bull eyes and 234C using the subcostal, costal and right parasternal border.
7- RWMA are related to strain. Hypokinesia and akinesia gives low strain result and you will ameliorate your strain analysis by doing more focus apical views.
8- This test could be use in cardiac MRI.
9- Do this test as a challenge you should have fun doing it and on long term you will save time and gain confidence.
PS.: Special thanks to DR Maria Di Lorenzo cardiologist, DR Caroline Ranger emergency physician and M. J. Boudreau-Béland for their precious help.
Real Lebeau, MD.
Cardiologist
Hôpital Sacré–Coeur
Montreal, Canada


The 6 images view
Analysis is the best way to understand the 3 minutes concordance test.
Question: Your diagnostic?
|
|
|
|
|
|
|
|
Answer:
Complement to ¨¨A systematic approach to LV short axis¨¨ Twelve techniques to find LV short axis.:
1- Classical technique (CLARRIS)
A) First for base and mid LV short axis. Starting from LV long axis you turn 90 degree to obtain mitral valve level and angulate downward to catch papillary muscle level.
B) Second for mid and apex short axis you start with short axis papillary muscle and angulate downward to have short axis of LV apex.
C) Focus technique (LARRIS) (cf A systematic approach...)
2- Lateral wall
3- Anterior wall
4- Right Ventricule 2 Chambers
5- Right Ventricule long axis with left vent.
6 -Inferior wall
7- Septal wall
8- Para apical technique (cf .: Horizontal LV technique)
9- Apical technique
10- Costal technique
11- SubCostal technique
12- Right parasternal technique
|

|
1- Right shoulder orientation
2- Left shoulder orientation
3- Liver orientation
4 –Spleen orientation
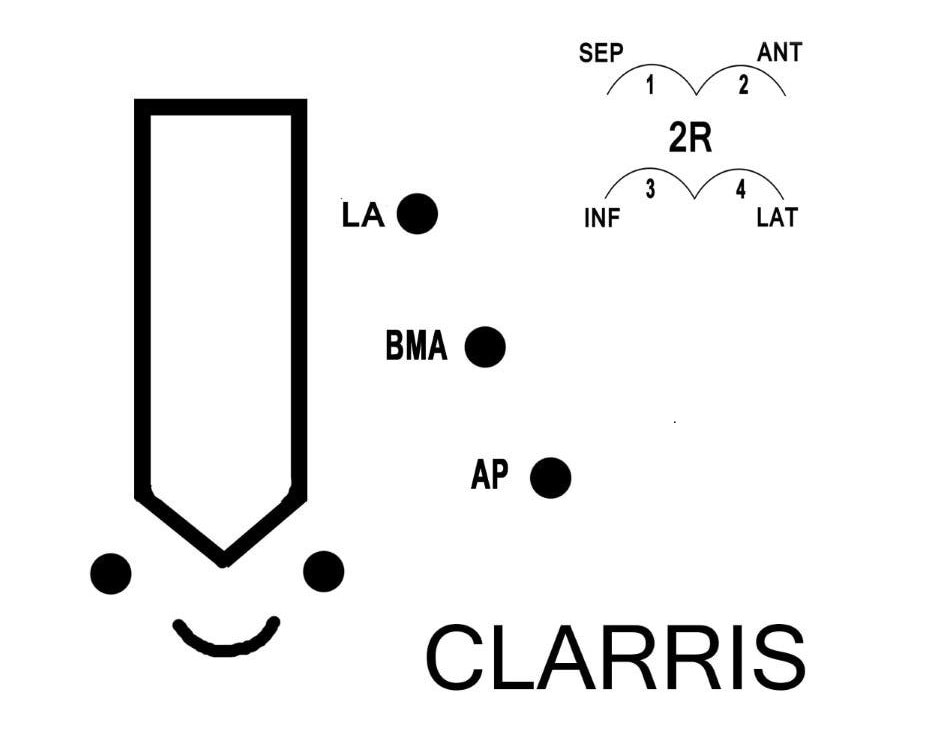
LA= long axis (classical technique)
BMA= Base Mid Apex (ballerina technique)*
AP= Apical